Vascular wall inflammation can affect both arteries (= high pressure vessels that transport blood from the heart to the organs) and veins (= thin-walled vessels that carry blood back to the heart).
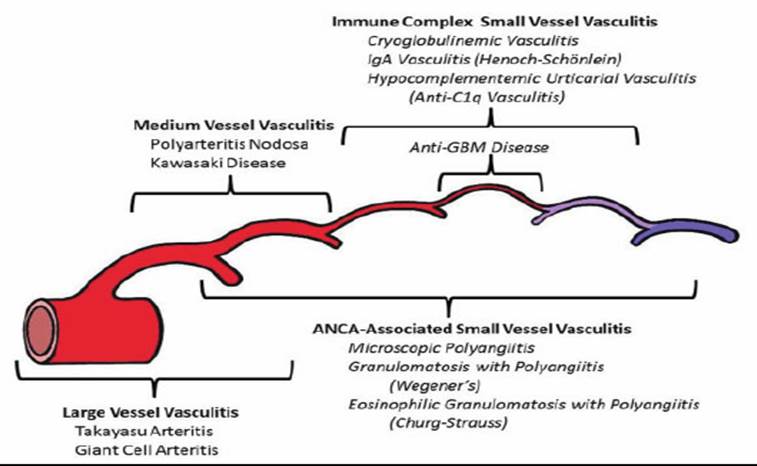
The classification of the diseases is primarily based on the size of the vessels, for example there is the group of “large vessel vasculitis” or the group of “small vessel vasculitis”.
A further subdivision is based on disease characteristics, for example the presence of ANCA antibodies in the blood, known as ANCA-associated vasculitis (AAV).
Representation of the vascular tree according to Chapel Hill:

Giant cell arteritis (GCA) is an inflammation of the vessel wall of medium-sized and large arteries.
It affects older people from the age of 50, with a steady increase in the likelihood of developing the disease into old age.
There are three forms of RZA: the best known is inflammation of the temporal artery (known as temporal arteritis), which leads to new types of headaches, usually on one side of the head, in the temporal region.
Other typical symptoms are visual disturbances such as double vision, distorted vision, color vision and blindness
Other symptoms
The second form is known as “polymyalgia rheumatica”. This manifests itself in muscle pain in the shoulder girdle and pelvic girdle. Those affected feel ill and completely stiff in the limbs, especially in the morning; for example, they can barely lift their arms to shoulder height. This form of the disease can occur with or without blood vessel involvement.
The third form is an inflammation of the vessel wall of the aorta and the large arterial vessels in the chest and abdomen (so-called large vessel vasculitis LVV). This form can occur without pain, but (almost) invariably leads to a strong feeling of illness, loss of appetite and weight and fever.
Diagnostics
In addition to the clinical examination, the investigations include visualization of the vascular inflammation by means of a tissue sample (so-called biopsy) of a temporal artery (minor surgical procedure), or by means of a new imaging examination:
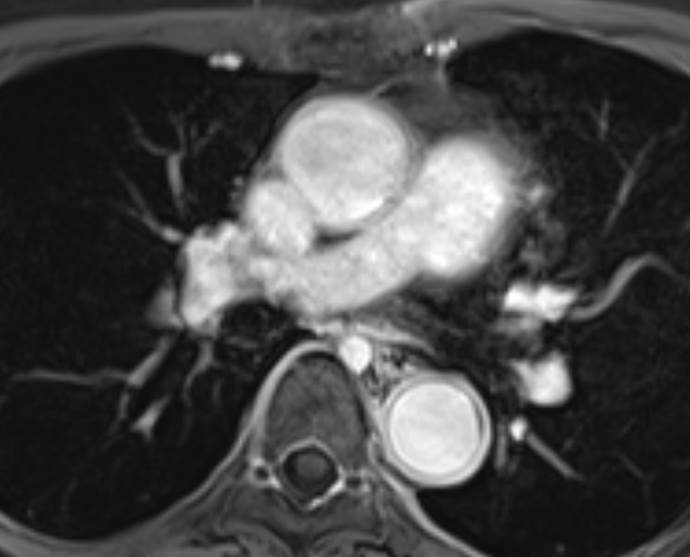
MR angiography: contrast agent accumulation in the vessel wall of the descending aorta, 10 minutes after injection of the contrast agent
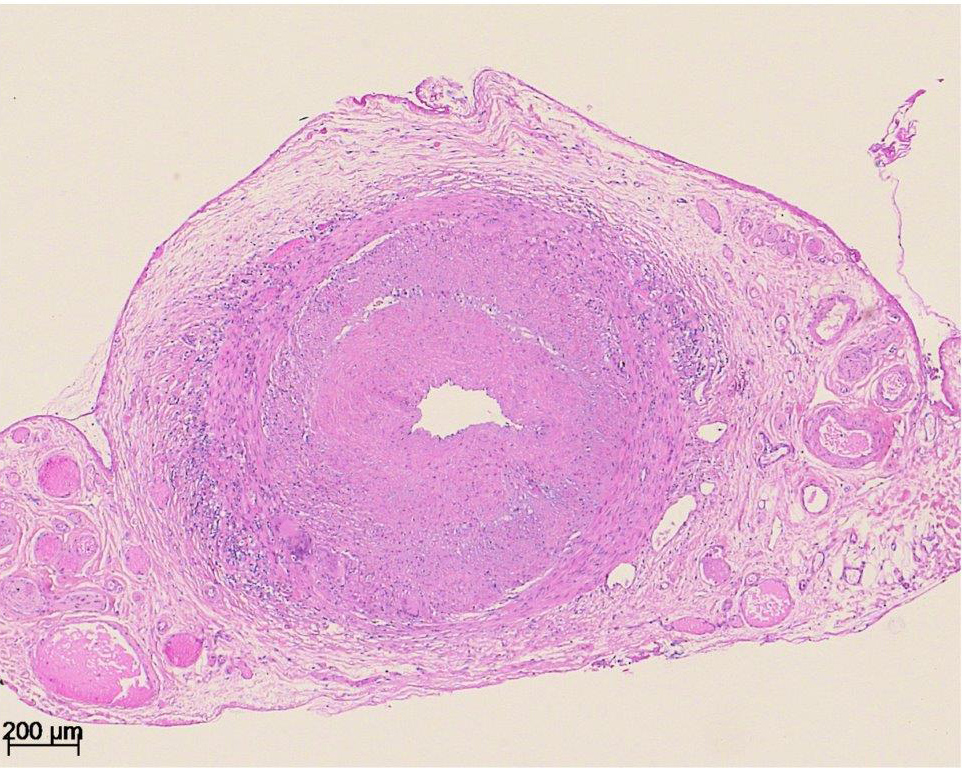
Biopsy: A typical histology of giant cell arteritis with thickening of the arterial wall, especially the intima, infiltration with mononuclear cells, formation of giant cells
Therapy
Immediate treatment with cortisone preparations (prednisone, Spiricort) is important to prevent possible blindness. In an emergency, contact one of the telephone numbers / addresses of the VASAS in your region!
As cortisone preparations (= glucocorticoids) always lead to undesirable effects such as bone loss (osteoporosis), muscle weakness, skin bleeding (especially on the back of the forearm), etc., the possibility of immunotherapy with tocilizumab or methotrexate should be examined. Both drugs are approved in Switzerland. If necessary, ask your family doctor for a referral to a specialist (e.g. a VASAS specialist).
Takayasu arteritis (TAK) is a very rare disease in which inflammation of the aorta and the medium and large arterial vessels occurs for an unknown reason.
The disease usually begins in childhood or young adulthood. Women are affected much more frequently than men. In Switzerland, the diagnosis is made with an average delay of 9 years. Symptoms include tingling, a feeling of weakness and/or coldness in the arms and legs, pain above the carotid artery, dizziness, visual disturbances and migraines, as well as abdominal pain.
Tiredness, poor performance and a slightly elevated temperature or fever are often complained about and often interpreted as psychological. Due to these unspecific symptoms and the absence of pain, the diagnosis is only made when a load-dependent paralysis of an arm occurs (for example when swimming or doing overhead work such as hanging objects).
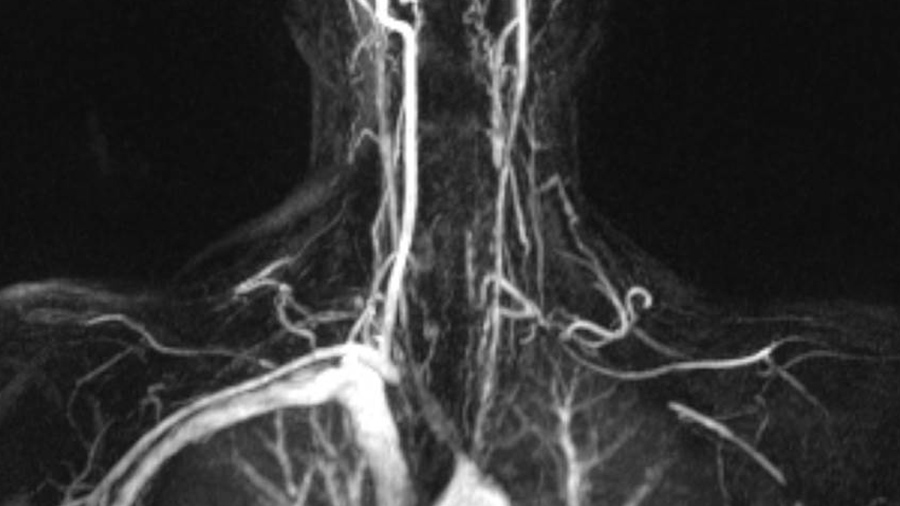
The usually only slightly elevated inflammation values in the blood test are striking (CRP repeatedly elevated, but only slightly above the norm in each case), other values normal) The suspicion is confirmed by an imaging examination, analogous to the examination of giant cell arteritis.
Copy of the RZA
Additional picture of me (pv)
Due to the young age of the patient, attempts are made to administer glucocorticoids (cortisone preparations) for as short a time as possible and to use immune preparations such as azathioprine or biologics such as infliximab from the start of treatment (reference Tak study)
Frequently prescribed remedies are:

In contrast to RZA and TAK, ANCA vasculitis affects the small vessels. In contrast to large vessel vasculitis, individual organs such as the kidneys or lungs can be severely affected in ANCA vasculitis. If left untreated, severe kidney dysfunction with dialysis (= kidney replacement procedure) can occur within a short period of time. While TAK affects young people and RZA affects older and elderly people, ANCA vasculitis typically affects people around the age of 50. However, children and the elderly can also develop the disease.
ANCA-associated vasculitis (AAV) is a group of three diseases (see also figure in the classification).
The term ANCA means that a blood protein, a so-called antibody, is often found in these forms of vasculitis, which is directed against the body’s own substances in white blood cells (ANCA = anti-neutrophil cytoplasmic antibody). This antibody plays an important role in the development of the disease.
The first symptoms of GPA usually occur in the nasal and sinus area. The inflammation leads to secretions, often bloody, and travels along the airways into the lungs. If other organs such as the kidneys or the nervous system are affected, ANCA is practically always detectable (so-called ANCA-positive vasculitis)
eGPA typically develops on the basis of an allergic bronchial disease. If the glucocorticoid-containing nasal sprays are no longer sufficient and treatment with prednisone tablets is necessary, this may be a sign of the onset of eGPA.
MPA is the most insidious form of AAV, as it lacks warning symptoms such as asthma or chronic nasal and paranasal sinus inflammation. It is also insidious because the kidney is affected and does not cause any symptoms such as pain or signs of inflammation.
The investigation of AAV includes blood and urine tests and a systematic examination of all organ systems. If at all possible, a tissue sample is taken (in the case of kidney infestation from the kidney, otherwise also from the skin or lungs). Rapid therapy is also important here, but it is very differentiated and depends on organ involvement, disease activity, prognostic factors and age.
Behçet’s syndrome (BS) is a chameleon. With classic clinical presentation, BS is easy to diagnose, but with atypical disease it can be delayed for years (see BS reference). BS can affect all types of vessels, from large arteries to medium and small vessels to large veins such as the vena cava of the trunk.
The NB also has a peculiarity that is important in terms of therapy, namely the so-called pathergy phenomenon. This describes the fact that even a minor trauma such as a pinprick can trigger a local inflammation. This characteristic can have serious consequences for vascular operations, as untreated vascular operations almost always lead to serious complications and re-operations.
The article on BS in Switzerland provides informaytion on organ participation and complaints (tables from the SMW publication)